
There is more than one way to eat a low carb ketogenic diet, in fact there are many variations. In this article I will outline three approaches including (1) a very high protein, similar to a Paleo diet as promoted by Dr. Ted Naiman and Dr. Tro Kalayjian (2) a high fat approach, as promoted by Dr. Jason Fung and (3) a higher protein lower fat intake during weight loss, then a moderate protein high fat intake during weight maintenance, as promoted by Dr. Stephen Phinney and Dr. Jeff Volek.
Three Types of “Low Carb” Diets
1 – Very High Protein
One proponent of a very high protein lifestyle is Dr. Ted Naiman, a board-certified family medicine physician who practices in Seattle, Washington. His videos on the subject of insulin resistance filmed at low carb conferences had a profound impact on me when I first adopted a low carb lifestyle in March of last year. This is something he wrote on Twitter today;
You can’t reduce carbs unless you first target protein so you aren’t hungry. If I tell a patient to stop eating carbs, they are starving and eat a whole box of Oreos—BUT if they eat a pound of steak and eggs, ok now carb reduction is easy!
Dr. Ted Naiman (@tednaiman), Twitter, January 16 2018, 11:06 PM
On the popular low carb site, Diet Doctor, Dr. Naiman oulines how much fat a person should eat on a ketogenic diet[2], depending on whether they are doing it for weight loss or weight maintenance. For someone seeking fat loss, Dr. Naiman recommends ~120 gm of protein, ~30 gm of net carbs, ~120 gm of ‘whole food fats’ (fat found naturally in food) and ~30 gm of added fat (such as for vegetables, salads and cooking).
His summary on Twitter is;
” target protein first (1 g per pound of DESIRED/ideal body weight), keep net carbs low, and eat whole food fats but avoid added fats if you are already fat or trying to get leaner. Nothing else even makes any sense.”
So, assuming someone’s ideal body weight is 120 lbs. How how much food does one have to eat to get 120 gm of protein? A lot as you’ll see below.
Another proponent of a high protein approach is Dr. Tro Kalayjian, a board certified Internal Medicine physician who currently practices in Greenwich, Connecticut. He lost 145 pounds over a two year period following a very high protein diet and like Dr. Naiman does a great deal of high intensity interval training (HIIT) and resistance training (RT).
When asked yesterday on Twitter whether he followed a high fat or high protein diet, he replied;
I’d say my only focus is to hit my protein target. I shoot for 200-350 g depending, especially if I do RT. With regards to fat, I eat plenty. I trim meats and don’t eat skin, but i eat variety of nuts from time to time and use olive/avocado oil.
Dr. Tro Kalayjian (@Dr.T), Twitter, January 15, 2018, 7:03 PM
Note: this is Dr. Kalayjian's plan for himself and not necessarily what he'd recommend for everyone. He does ~10 hours of HIIT and RT training a week, with a goal of increasing muscle mass (hypertrophy) and re-composition. What Dr. Kalayjian would recommend to others depends on (1) what their goal is, (2) what their current medical/metabolic status is and (3) any lifestyle details that will impact dietary requirements.
How much actual protein is in what we call ‘protein foods’? Here are some examples;
Egg (1 large) – 6.3 grams
Sausage, pork link (14 gm / 0.5 oz each) – 2.5 grams
American cheese (28 gm / 1 oz.) – 7 grams
Cottage cheese (250 ml / 1 cup) – 28.1 grams
Salmon (170 gm / 6 oz.) – 33.6 grams
Ham (170 gm / 6 oz.) – 35.4 grams
Tuna (170 gm / 6 oz.) – 40.1 grams
Chicken, breast (170 gm / 6 oz.) – 37.8 grams
Broiled Beef steak (170 gm / 6 oz.) – 38.6 grams
Hamburger (170 gm / 6 oz.) – 48.6 grams
Turkey, dark meat (170 gm / 6 oz.) – 48.6 grams
Pork Chop (170 gm / 6 oz.) 49 grams
Beef (170 gm / 6 oz.) – 54 grams
So, what would Dr. Kalayjian’s daily intake of 200-350 gm. of protein look like in terms of food? Let’s look at how much food is need to eat meet only 200 gm of protein per day, which is the ‘low end’ of Dr. Kalayjian’s intake;
Three eggs at breakfast would only supply less than 19 gm of protein.
Four pork link sausages would supply another 10 gms of protein.
He’d only have eaten less than 30 gms of protein.
Eating a 340 gm (12 oz) broiled beef steak at lunch-time would add another 77 gms of protein.
After these two meals, he would have eaten 106 gms of protein and be only a little over half-way to his minimum protein goal and less than a third the way to his upper range of protein.
Let’s say he decided to eat 1/2 a large salmon i.e. 340 gm (12 oz) for supper, that would add 67 grams of protein.
Adding up all the protein so far, he would have only eaten 173 gms of protein, so he’d have to fry up 4 more eggs to make his 200 gm of protein to meet his minimum protein requirement.
Looking back to Dr. Naiman’s “pound of steak and eggs“, let’s break that up over a day. Three eggs for breakfast would supply <20 gm of protein and eating 227 gm (8 oz) of beef at lunch would provide 50 gm of protein, so the person would need to eat another 227 gm (8 oz) of beef at supper just to make their 120 gm of protein for the day. Now, remember, this is for an individual whose ideal body weight is only 120 pounds! That is a lot of meat and eggs.
This approach should really be dubbed “low carb high protein (LCHP)” as that’s what it is. It may be appealing for those doing body building and body sculpting but is eating high protein (i.e. 120 gm per day), as Dr. Naiman proposes, appropriate for people seeking fat loss?
As mentioned above, I think it would depend on (1) the goals and (2) medical/metabolic status of an individual, and (3) whether there are any lifestyle factors that impact dietary intake. There is also the matter of “human protein tolerance” and the effect of high protein intake on ketosis, outlined below.
2 – High Fat
One of the popular proponents of a high fat approach is Dr. Jason Fung, a Toronto-area nephrologist (kidney specialist). His approach is reflected in the blogs he has been writing since 2013 as part of the Institute of Kidney Lifescience Technologies (www.kidneylifescience.ca), which have since become the basis for his Intensive Dietary Management (IDM) Program, based out of Toronto[4].
From what I gleaned back from my early days reading all of his first two years of his blogs (Aug 2013- May 2015) and many since, Fung promotes a diet which is a maximum of 20-30 gm of net carbohydrate (gross carbohydrate content minus fiber) per day, a maximum of 75 gm of protein per day (~20 gm of protein at each meal), with the remainder of intake as a variety of fats. Fung does not promote the use of “fat bombs” popularized with the “Bulletproof Diet”, but encourages the eating of fat that comes naturally in food; such as the skin on poultry, the visible fat on meat and the yolk of eggs plus a total of 70 gm of added fat per day for satiety (feeling full).
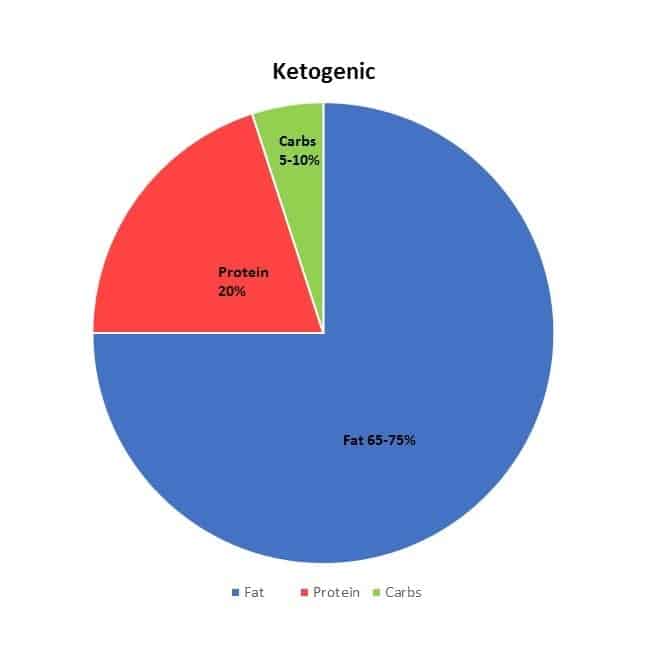
More recently, Dr. Fung’s recommendations seem to be closer to the classic ketogenic diet which is lower in carbs (5-10% net carbohydrate) with about the same amount of fat and same moderate protein intake.
Fung does not recommend the adding excess fat (“fat-bombs”) to the diet, made popular by the “Bulletproof Diet” written by layman “biohacker” Dave Asprey.
Also fundamental to Fung’s approach is the use of Intermittent Fasting to restore insulin sensitivity, which ultimately also has the effect of decreasing overall intake.
- a 16-hour fast begins from the end of supper the previous night, until lunch the following day. That is, only breakfast isn’t eaten.
- A 24-hour fast begins from the end of supper the previous night, until supper the following day (i.e. one meal).
- A 36-hour fast begins from the end of supper the previous night and no breakfast, lunch or dinner is eaten the following day, with the fast broken at breakfast the next day.
- A 42-hour fast is like the 36-hour fast, except people fast until lunch on the day following the fast.
Fung’s “fasts” are not water-only fasts, but allow the drinking of ‘bone broth’ during fasting periods, amongst other beverages.
3 – Higher Protein Lower Fat followed by Moderate Protein High Fat
Dr. Stephen Phinney MD, PhD, a medical doctor and Dr. Jeff Volek, RD, PhD a Registered Dietitian have decades of combined scientific and clinic research experience in the area of low carb diets and in 2011 published their expert guide titled The Art and Science of Low Carbohydrate Living [2] documenting the clinical benefits of carbohydrate restriction.
They promote a low carbohydrate diet that is higher protein during the weight loss phase only, but the level of protein they recommend is nothing near the levels that Dr. Naiman and Dr. Kalayjian encourage, but still as I will outline below, it still requires a large quantity of protein foods to be eat daily.
In the induction and weight loss phase using Phinney and Volek’s approach, protein is ~30% of caloric intake but decreases to ~21% of caloric intake following weight loss, during weight maintenance. Fat is 60% of calories during the weight loss phase and 65-72% during weight maintenance. Carbohydrate intake is kept very low (7.5-10% of calories for men, 2.5-6.5% of calories for women) and this induces nutritional ketosis.
The amount of mathematical calculations required for the average individual to follow Phinney and Volek’s method is, at the very least, daunting. The amount of fat in grams and carbohydrate in grams needs to be calculated initially during induction and recalculated for weight loss, then recalculated again during pre-maintenance and maintenance. In addition, as the person’s weight decreases, the number of grams of fat and carbohydrate also needs to be recalculated. The amount of protein that must be eaten on an ongoing basis is another challenge to their approach.
What does 100-150 grams of protein look like in terms of actual food [3]?
Two eggs at breakfast would only supply less than 13 gm of protein. Eating 170 gm (6 oz) of salmon at lunch-time would only supply less than 34 gm.
A woman would need to eat 2 additional hamburger patties (170 gm / 6 oz, cooked), or 170 gm / 6 oz of turkey or pork or beef in order to meet her daily protein requirement. A man would need to eat double that to meet his daily protein requirement.
Human Protein Tolerance
Ironically, even though Phinney and Volek encourage eating more protein than fat during weight loss, they write about “human protein tolerance“, including the “lethargy and malaise” that occurs when more protein than fat is eaten on a regular basis, along with the feeling of being “sick to the stomach” [3, pg. 210]. They also point out that there seems to be a physiological upper limit of protein intake of 20-25 gms per meal, after which skeletal muscle is no longer synthesized with additional intake.
Another reason Phinney and Volek recommend avoiding eating too much protein is that it lowers ketone production;
“it [protein] has a moderate insulin stimulating effect that reduces ketone production. While this effect is much less gram-for-gram- than carbohydrate, higher protein intakes reduce one’s keto-adaptation and thus the metabolic benefits of the diet.”
Phinney SD, Volek JS, The Art and Science of Low Carbohydrate Living: An Expert Guide, Beyond Obesity, 2011, page 210.
This Dietitian’s Approach
For the most part, my approach (for those without hereditary cholesterol or triglyceride issues) is closer to Dr. Fung’s approach than to either of the others, with some modifications.
One the modifications is around the types of fat that are central in the diet. Like Fung, I encourage people to eat fat that naturally comes with food (egg yolk, for example) but I don’t encourage the amount of saturated fat that his blogs reflect. I am fine with people eating eggs a few times a week (again, provide there are no clinical reasons not to), but I encourage my clients to consider rich sources of monounsaturated fats such as avocado, nuts and seeds and their oils as their primary fat source, with omega-3 poly-unsaturated fat from fatty fish such as salmon, tuna, mackerel and sardine, a close second.
Another modification that I have made is that I encourage my clients to eat cheese as it supplies a good source of calcium, that doesn’t have the anti-nutrients such as oxalates and phytates that are found in many calcium-rich vegetables.
For those that prefer to, I support clients that want to eat more protein during the weight loss phase (provided there is no clinical reason not to) but like Phinney and Volek, I adjust protein intake downward (~21-23% of caloric intake) after weight loss has occurred. In my experience, there are quite a number of my clients that started out wanting to eat high protein, but quickly found out that when they eat more protein than fat, they feel nauseated. This finding of feeling “sick to the stomach” was referred to above as documented by Phinney and Volek and came from a study of prolonged meat diets in the early 1930’s. It is also supported from the traditional indigenous diets of the Inuit which Phinney and Volek point out “keep their protein intake moderate to avoid the lethargy and malaise that would occur if they ate more protein than fat” [3].
There is no one “right” way to eat a low carb, ketogenic diet. What works for weight loss often comes down to what a person can easily do long-term. Whether that is moderate protein or higher protein isn’t as significant, because in the end both Fung’s approach and Phinney and Volek’s weight maintenance approach are almost identical; 70-75% fat, 7.5-10% carbohydrate and 21% protein.
Everyone is different and there isn’t a “one-size-fits-all” low carb approach.
As well, no Meal Plan is ‘carved in stone’. Sometimes for reasons of preference or clinical reasons, a client may start out with a higher fat approach but as they get closer to their goal weight, it may become necessary to reduce the amount of fat intake, so that they can take off the remainder of the weight.
I make the process easy.
After conducting a thorough assessment, I do the math required to design their Meal Plan, calculating their protein requirement based on their physiological needs as well as the low carb approach they’ve chosen, then distribute their fat and carbohydrate intake around that.
As people lose weight, their Meal Plan can be adjusted if need be and if their weight loss has plateaued or their insulin resistance isn’t decreasing sufficiently, then we’ll consider together adjusting the amount of carbohydrate downwards.
Have questions?
Please send me a note using the “Contact Me” form above.
References
1. Mark’s Daily Apple, How to Eat Enough Protein, April 3, 2008 URL: www.marksdailyapple.com
2 – How Much Fat for a Ketogenic Diet; maintenance versus fat loss, https://www.dietdoctor.com/much-fat-eat-ketogenic-diet
3. Volek JS, Phinney SD, The Art and Science of Low Carbohydrate Living: An Expert Guide, Beyond Obesity, 2011
4. Fung, Jason, Institute of Kidney Lifescience Technologies (www.kidneylifescience.ca) & Intensive Dietary Management (IDM) Program (www.intensivedietarymanagement.com)
OnKeto.com is a news aggregation service that brings you best of world articles to you for your consumption.
Author: None
Author URL: None
Original Article Location: http://www.lchf-rd.com/2018/01/16/which-low-carb-ketogenic-diet-high-fat-high-protein-or-a-mixture/